AC joint pain
This article is about inflammation, arthritis and overuse of the AC joint – for sudden impact and trauma to the AC joint click here
What is the AC joint?
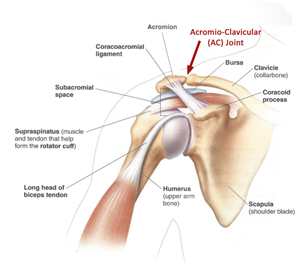
The shoulder is a very complicated structure consisting of three bones (shoulder blade, collarbone and arm) that all move together. The AC joint is the small joint between the shoulder blade and the collar bone
What is AC joint pain
In my experience many (if not most) cases of AC joint pain are first wrongly diagnosed as ‘impingement,’ ‘bursitis,’ ‘swimmers shoulder’ or ‘supraspinatus tendonitits’. This is a shame because AC joint pain is often usually very easy to treat. Often there will be pain lying on the effected side, reaching across or behind your body and performing pushing or lifting movements.
Why does AC joint pain occur?
I most people, the AC joint is the first joint in their body to start developing ‘wear and tear’ and this can happen before the age of 30! Thankfully, it is not a weight-bearing joint and we can usually tolerate that damage without too much trouble. Sometime, particularly with swimming, paddling and weight-training, that ‘wear and tear’ can spark of excessive inflammation which can quickly escalate.
How is AC joint pain diagnosed?
Most cases of AC joint pain can be diagnosed by an expert Sport and Exercise Physician without the need for scans. It is important to realise that sometimes scans (like an ultrasound) can even lead us in the wrong direction and many people with AC joint pain are told that their scan shows bursitis which is not always relevant to their pain.
How is AC joint pain treated?
The most important factor for treating AC joint pain is getting the diagnosis right in the first place. Sometimes rest, modified activities and oral anti-inflammatories can work well but often a corticosteroid injection (cortisone) is required. Cortisone is just a strong, locally active, anti-inflammatory that is effective in breaking that vicious cycle of inflammation. In most cases the AC joint return to having some mild wear and tear that is not painful or limiting and no further treatment is required. If cortisone is only partially or temporarily effective, then it is possible (in a minority of cases) that surgery could be required. The surgical procedure is done by a minimally invasive key-hole approach and has excellent success rates.